Microscope histological image of IBD colitis intestine
Relate drug response to clinical history
Precision medicine aims to deliver the right drug to the right patient at the right dose. However, most presently available drugs fail to work in a high percentage of patients; including treatments for IBD.3 At REPROCELL, we offer early-stage characterization of the patient population. By combining measurements of drug efficacy with clinical histories and access to state-of-the-art molecular phenotyping, we can investigate inter-individual variation in drug response at the preclinical stage.
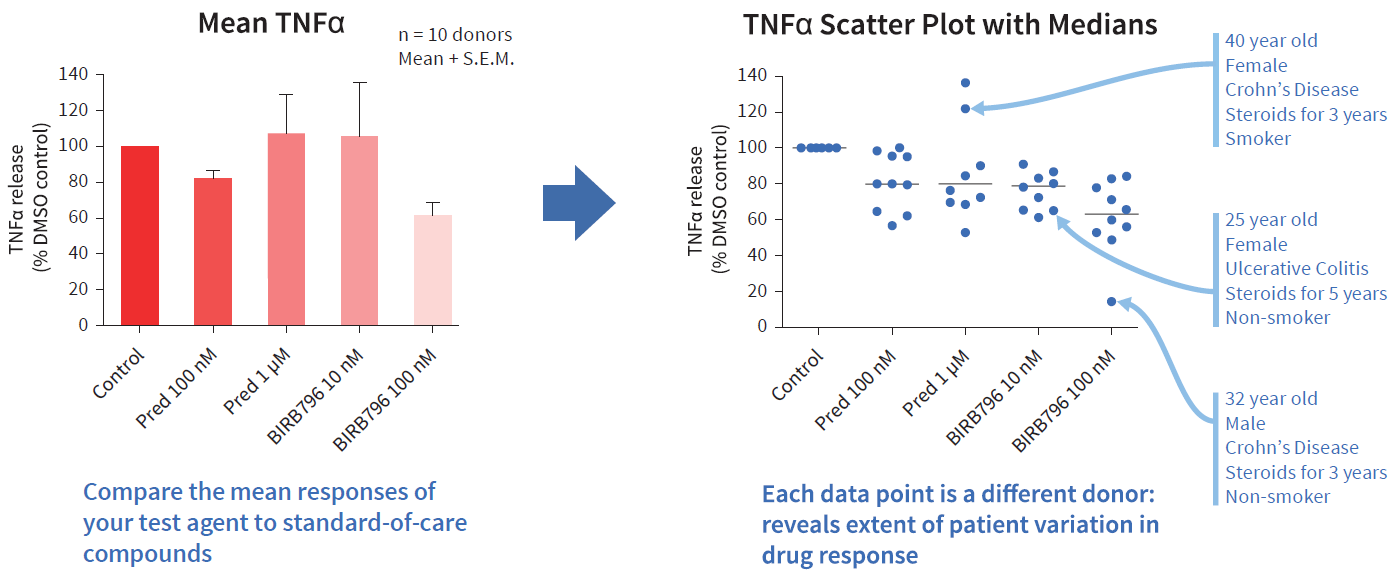
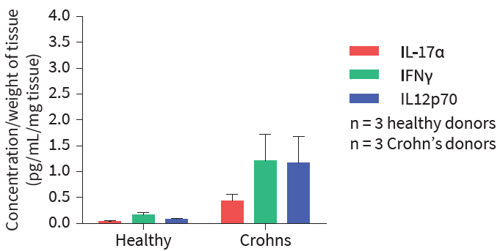
Figure 1: In this example, over 40 inflammatory mediators were measured to investigate the cytokine release profiles in healthy and diseased tissue. The disease group showed greatly increased levels of a range of key cytokines and chemokines commonly upregulated in IBD, including IL-17α, IFNγ and IL-12p70.
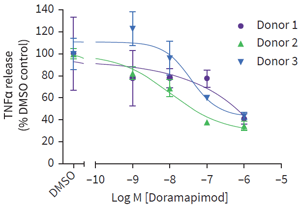
Figure 2: Intestinal biopsies were obtained from 3 UC patients. Following an 18-hour culture period, TNFα release was measured across a wide concentration range of the test agent Doramapimod (see graph). Differences in response were evident across patient samples, suggesting variation in the UC patient population, as is known to occur clinically.