
Cross-section showing the microscopic structure of the 3D IBD model before inducing an inflammatory response
Immune response
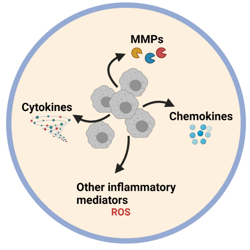
- Cytokine and chemokine production
- Inflammatory marker production
- Pro-inflammatory status
Barrier integrity
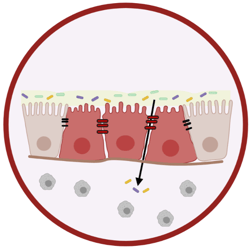
- Trans-epithelial resistance (TEER)
- Transport assays
- Histological assessment
- ICC/IHC staining
- Junction analysis
- Junction quantification by PCR and WB
- EM analysis
ECM remodelling
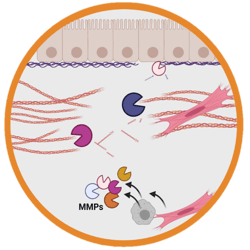
- ECM quantification
- ICC/IHC staining
- MMP/TIMP production
- Cytokine/chemokine production
- Marker quantification
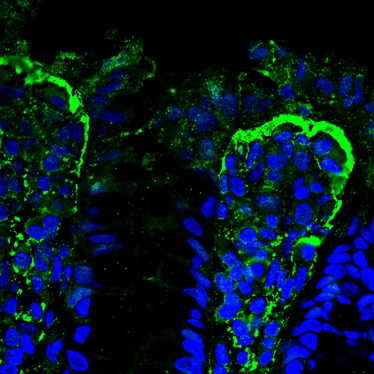
The IBD biomarker MMP-9 (green) accumulates at the epithelial/stromal interface of the 3D model, which is the same as can be observed in ulcerative colitis tissues of patients.
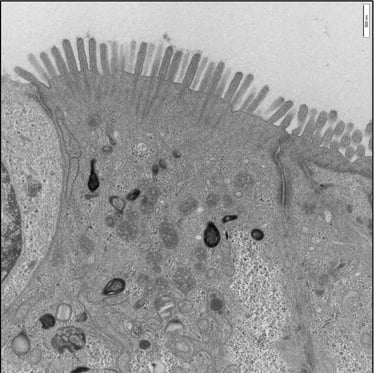
A confluent microvilli brush border is observed across the surface of the unstimulated 3D model, showing clear rootlet visibility.