
Why are PBMCs Important for Clinical Research?
In the context of increasingly complex clinical trials, peripheral blood mononuclear cells (PBMCs), a subset of cells within whole blood, can offer valuable insights into human biology. Alongside plasma and serum, PBMCs are a rich source of information for identifying immune-based diagnostic and prognostic biomarkers. Their use enables high-resolution immunophenotyping, allowing researchers to dissect intricate immunological mechanisms and signalling pathways that help predict the safety and efficacy of immunotherapies.
One of the key advantages of PBMCs is that they provide a snapshot of an individual’s immune status at a specific point in time. They support a broad spectrum of experimental approaches, ranging from cellular assays to multi-omics analyses, and are integral to several downstream clinical applications, including biomarker discovery, vaccine development, and adoptive cell therapies (Figure 1). 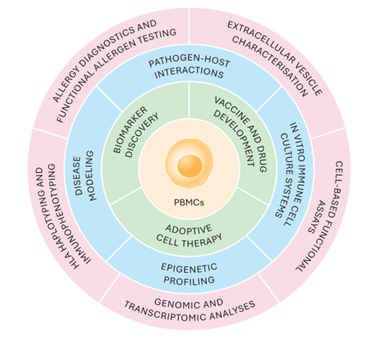
Figure 1. Downstream applications of PBMCs
Once isolated, these cells can be cryopreserved, retaining their viability and functionality for future analyses. This flexibility is particularly valuable in longitudinal studies and large multicentre trials, facilitating consistency across both time points and geographic locations.
Challenges in Multi-site Clinical Trials
One of the major hurdles in modern clinical trials is coordinating activities across geographically dispersed investigator sites. Trials often span multiple regions to ensure a representative cohort; however, this geographic range introduces challenges in harmonising blood specimen collection and PBMC isolation across sites. Differences in equipment, staff expertise, and procedural execution can lead to technical variability, ultimately affecting data quality.
PBMCs are particularly sensitive and can begin to deteriorate ex vivo within 24 hours of blood collection. Inconsistencies in specimen handling, transport or processing can significantly impact cell yield, viability, and functional integrity. As a result, the reproducibility of downstream applications and the reliability of clinical trial data may be compromised.
Careful management and monitoring of every stage — from collection through shipment, isolation and storage — are therefore essential to ensure data integrity, reproducibility, regulatory compliance, and confidence in clinical outcomes.
Choosing the ‘Right’ PBMC Isolation Method
There is no one-size-fits-all protocol for PBMC isolation. Different clinical trials present unique requirements depending on the therapeutic context and intended downstream analyses. While organisations such as the Office of HIV/AIDS Network Coordination (HANC) have established standardised guidelines, individual studies often require tailored approaches to meet specific scientific and regulatory needs.
Selecting and standardising the right PBMC isolation method is critical to controlling process variation and ensuring reliable immunological assessment. Key considerations include cell yield, purity, viability, immunogenic potential, compatibility with downstream applications, and cost. Importantly, uniform implementation across all study sites is essential for comparability.
Density gradient centrifugation remains one of the most widely used techniques. First described by Böyum in 1968, this method exploits the distinct density profiles of blood components, enabling separation of PBMCs into a defined layer (the “buffy coat”) between the plasma and the density gradient medium following centrifugation. (Figure 2). Denser cells, such as red blood cells and granulocytes sediment to the bottom while less dense elements congregate in the plasma component.
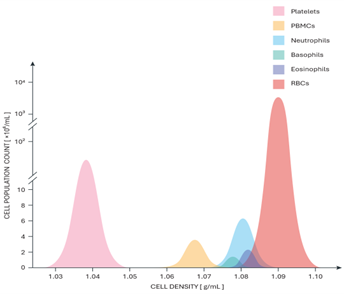
Figure 2. Densities of various cell types in the human blood
Cellular components stratify according to density. PBMCs, including monocytes, T and B lymphocytes, natural killer (NK) cells, dendritic cells, and haematopoietic progenitors, accumulate in the ‘buffy coat layer.
Adaptations of the technique have been developed to improve efficiency and standardisation (Table 1). For example:
- Fritted barrier tubes (e.g. Accuspin™, SepMate™, LeucoSep™) streamline the process by reducing manual steps and minimising variability. A porous barrier separates the density gradient medium from the blood sample to ensure an improved layering step.
- Cell Preparation Tubes (CPTs)offer a closed system with pre-filled anticoagulant and separation medium, enabling simplified on-site processing.
- Semi-automated methods, such as magnetic-activated cell sorting (MACS), allow targeted enrichment of specific PBMC subsets.
- Fully automated microfluidic platforms support high-throughput processing with reduced hands-on time, particularly valuable in clinical-scale cell manufacturing applications.
The choice of anticoagulant is another critical factor. Different anticoagulants have distinct physicochemical properties that can influence immune cell activity and assay performance. For instance, EDTA may reduce PBMC immunogenicity, impair T cell activation, and suppress NK cell cytotoxicity, whereas heparin (potassium, sodium, or lithium salts) is generally preferred when processing delays are expected due to its ability to better preserve cell function.
Table 1. Different PBMC isolation methods
| Density Gradient Medium | Fritted Barrier Tubes | Cell Preparation Tubes | Immunomagnetic Cell Separation | Microfluidic-Based Cell Separation | |
| Technology | Ficoll overlay in the standard centrifuge tube | Accuspin. SepMate, LeucoSep | Closed cell separation systems with different anticoagulants | RoboSep, EasySep, MACS Cell Separation | CTS Rotea, Sepax C-Pro, Elutra, Lovo, CliniMACS Prodigy |
| Advantages | Standard | Easier to standardise, decreased processing time | On-site processing. Significantly reduced processing time | Semi-automated, immune cell enrichment, rapid | Fully automated, high-throughput, easy to use, versatile, high-purity |
| Disadvantages | Intra and inter-operator variability, Time-consuming | Reduced PBMC yields compared to standard |
Higher possibility for contamination |
More expensive, less available, special kits | Extremely expensive, less available, specialised training needed, special consumables |
Standardising and Controlling Process Variability
PBMCs have played a pivotal role in clinical research for decades, enabling real-time monitoring of immune responses and supporting adaptive treatment strategies. However, minimising non-specific variation associated with PBMC processing remains essential. Even small inconsistencies can compromise downstream analyses and clinical outcomes.
The PBMC lifecycle typically begins at the investigator site with whole blood collection, followed by processing either on-site or at a central laboratory. The resulting cells are cryopreserved under tightly controlled conditions to preserve viability and function for future use (Figure 3). Each point in the life cycle is open to variability that may affect the process outcome.
 Figure 3. Major sources of technical variation in PBMC processing
Figure 3. Major sources of technical variation in PBMC processing
a. Investigator Site Best Practice
Investigator sites are responsible for subject recruitment and specimen collection in accordance with study protocols. This includes adherence to specific requirements, such as the type and order of blood collection tubes and the timing of sample collection. Deviations from these protocols can introduce variability at the earliest stage of the process.
Important considerations include:
- Venepuncture technique — poor handling can lead to haemolysis (rupture of RBCs to release haemoglobin), reducing sample quality. Improper handling may include excessive agitation, inadequate mixing, inappropriate needle gauge or prolonged tourniquet application.
- Scheduling blood collection — delays between collection and processing can significantly reduce cell viability. Ideally, blood specimens should be processed within a few hours of collection. In practice, however, delays are common, particularly when investigator sites lack on-site PBMC processing capabilities.
- Staff training and quality assurance — regular training and robust quality systems help ensure consistent adherence to protocols.
b. Shipment and Logistics
Timely and controlled shipment of blood specimens is critical. Ideally, samples should be processed within a few hours of collection; however, in multicentre trials utilising central laboratory services, transit times of 24 hours or more are common.
Extended transport times, combined with temperature fluctuations outside the optimal range (18–25°C), can negatively affect PBMC viability and function. Delays may lead to altered cytokine kinetics, reduced lymphocyte activity, and cellular degradation. To mitigate these risks, validated transport conditions, specialised courier services, and temperature monitoring systems should be implemented.
c. Laboratory Processing
Laboratory processing is a critical step in achieving successful PBMC isolation. Even minor variations can have a significant impact on downstream analyses, making validated and well-controlled processes essential.
Upon receipt, samples must be logged in accordance with good clinical laboratory practice (GCLP), ensuring accurate identification and traceability. Missing or incorrect information can render samples unsuitable for analysis and lead to delays.
PBMC processing typically involves four stages: blood dilution, density gradient centrifugation, cell recovery and counting, and cryopreservation. Key technical considerations across these stages include:
- Use of appropriate buffers to support cell stability and prevent clumping. Calcium- and magnesium- free salt solutions incorporating a protein carrier, for example, can assist enzymatic function and prevent cell loss during the process.
- Optimised centrifugation parameters to ensure effective separation. Density gradient medium selection and handling, acceleration and deceleration speeds, and prolonged protocols can interfere with the efficiency of cell separation.
- Accurate cell counting methods to ensure consistency. Manual counting offers precision and nuance whilst automated counting options offer speed, consistency and reproducibility for higher through-put workflows.
- Gentle handling to prevent cell damage or unintended activation. Harsh handling, such as excessive pipetting or abrupt centrifugation cessation may cause immune cell activation or lysis of more fragile subsets
d. Cryopreservation and Storage
Cryopreservation is essential for maintaining PBMC viability and functionality. An optimal cryoprotectant with controlled freezing followed by storage in ultra-low temperature conditions ensures long-term stability. Proper cold chain management and inventory control systems are critical for maintaining sample integrity and traceability throughout the study lifecycle.
e. Quality Control and Assurance
Reliable PBMC isolation depends on consistent execution and robust quality assurance systems. Method validation, staff training, facility and equipment maintenance are central components of these systems. Internal quality control measures monitor key indicators such as cell viability, recovery rate, processing time, and cryopreservation quality.
External quality assurance programmes complement these measures through operator training, proficiency testing, and regulatory audits, ensuring consistency across sites and adherence to established standards.
Conclusion
The isolation and processing of PBMCs is a critical, yet often underestimated, component of clinical trial success, particularly in complex, multi-site studies. Variability introduced at any stage — whether during specimen collection, transport, or laboratory processing — can significantly impact both sample integrity and the reliability of downstream analyses.
References
- Riedhammer C, Halbritter D, Weissert R. Peripheral blood mononuclear cells: isolation, freezing, thawing, and culture. Methods Mol Biol. 2016;1304:53–61. https://doi.org/10.1007/7651_2014_99.
- Dinh B, Hoeksema MA, Spann NJ, Rendler J, Cobo I, Glass CK, Yeang C. Isolation and cryopreservation of highly viable human peripheral blood mononuclear cells from whole blood: a guide for beginners. J Vis Exp. 2024;(212). https://doi.org/10.3791/66794.
- Betsou F, Gaignaux A, Ammerlaan W, Norris PJ, Stone M. Biospecimen science of blood for peripheral blood mononuclear cell (PBMC) functional applications. Curr Pathobiol Rep. 2019;7:17–27. https://doi.org/10.1007/s40139-019-00192-8.
- Lehle S, Völkl S, Seitz K, et al. Effect of delayed isolation of peripheral blood mononuclear cells on cell viability and functionality. BMC Immunol. 2025;26(1):21. https://doi.org/10.1186/s12865-025-00701-y.
- HIV/AIDS Network Coordination (HANC). Cross-Network PBMC Processing SOP v7.0. Published online. Accessed August 2025. Available at: https://www.hanc.info/content/dam/hanc/documents/laboratory/cross-network-procedures-sops/Cross-Network%20PBMC%20Processing%20SOP%20v7.0.pdf
- Bahunde F, Neidinger E, Awoyode R, et al. Evaluation of PBMC processing in the Precision Bioservices laboratory network (HUM7P.325). J Immunol. 2014;192(Suppl 1):184.34. https://doi.org/10.4049/jimmunol.192.Supp.184.34.
- Becza N, Yao L, Lehmann PV, Kirchenbaum GA. Optimizing PBMC cryopreservation and utilization for ImmunoSpot® analysis of antigen-specific memory B cells. Vaccines (Basel). 2025;13(7):765. https://doi.org/10.3390/vaccines13070765.
- Weinberg A, Song L, Wilkening C, et al. Optimization and limitations of use of cryopreserved peripheral blood mononuclear cells for functional and phenotypic T-cell characterization. Clin Vaccine Immunol. 2009;16. https://doi.org/10.1128/CVI.00342-08.
- Yang J, Diaz N, Adelsberger J, et al. The effects of storage temperature on PBMC gene expression. BMC Immunol. 2016;17:6. https://doi.org/10.1186/s12865-016-0144-1.
- Jerram A, Guy TV, Beutler L, et al. Effects of storage time and temperature on highly multiparametric flow analysis of peripheral blood samples: implications for clinical trial samples. Biosci Rep. 2021;41(2):BSR20203827. https://doi.org/10.1042/BSR20203827.

About the author
Dr Nikola Kolundzic, Analytical Project Manager and Study Director, REPROCELL Europe
Dr Nikola Kolundzic serves as an Analytical Project Manager for clinical laboratory projects and a Study Director for preclinical drug discovery, with a focus on dermatology research. His extensive expertise in pluripotent stem cells, tissue engineering, 2D and 3D cell culture, and skin disease modeling perfectly aligns with REPROCELL’s mission to develop robust, reliable, and high-throughput in vitro models for drug discovery and product development.
Subjects we write about
- 3D Cell Culture
- Cell Culture
- Central Lab Services
- Clinical Capabilities
- Disease Modeling
- Drug Discovery
- Gene Editing
- Genomic Services
- GMP
- Human Tissue Samples
- Human Tissue Testing
- IBD
- Life Sciences
- Master Cell Banks
- Neurons
- Oligonucleotide Synthesis
- Pharmacology-AI
- Precision Medicine
- Product Catalog
- Regenerative Medicine
- Respiratory Disease
- Safety Pharmacology
- Skin Disease
- Stem Cells
%20(1).png?width=400&height=225&name=New%20Approach%20Methodologies%20(NAMs)%20(1).png)
.png?width=400&height=225&name=New%20Approach%20Methodologies%20(NAMs).png)



