
Changes in uterine contractility are essential for regulating pregnancy and labor in humans.1 Several endogenous and exogenous substances can influence this process such as hormones, inflammatory mediators, and drugs. Natural or artificial inhibition of uterine contractility prevents premature delivery, while induction encourages labor.2,3
The role of uterine contractility in humans
During labor, uterine contractions change from episodic and uncoordinated events to highly-coordinated contractions that significantly increase intrauterine pressure.1 This change typically occurs at night, suggesting neural control.1 Uterine resting tone and amplitude are also increased during menses to help expel the womb lining and are thought to contribute to dysmenorrhea.3 We have listed several exogenous and endogenous compounds involved in uterine contractility and their effect below.
Compounds that promote human uterine contraction
Oxytocin: Oxytocin is thought to mediate the circadian rhythm of uterine contractility and is used clinically to induce and accelerate labor.1 Due to its contractile effects, oxytocin is commonly used as a control compound, or to induce contractions of uterine tissue during ex vivo testing.
Oxytocin-Oxytocin receptor
Determine whether your test article affects uterine contractility via oxytocin receptors.
Prostaglandins: The concentration of prostaglandins in the plasma and amniotic fluid increases during labor.3 These inflammatory mediators encourage myometrial contractions to induce labor.3 Prostaglandins are also related to the changes in gap junction formation and connexin-43 expression during labor.1
Vasopressin: Vasopressin has been used prophylactically in gynecological surgery for over 70 years for its vasoconstrictive properties.4 In pregnancy, the volume of vasopressin in the extracellular fluid increases to reduce the risk of post-partum hemorrhage.4 This hormone contracts the smooth muscle of the myometrium resulting in vasoconstriction, and prophylactic use can reduce blood loss during hysterectomy, myomectomy, vaginal, and cervical procedures.4 However, the cardiopulmonary side effects of vasopressin mean that caution must be exercised when using this drug clinically.4
Vasopressin-Vasopressin receptor
Determine whether your test article affects uterine contractility via vasopressin receptors.
Compounds that promote human uterine relaxation
Progesterone: The hormone progesterone is best known for its role in decreasing uterine contractility during the luteal phase of the menstrual cycle.5 It may also be involved in the changes in gap junction regulation that occurs during labor.1 Progesterone concentration decreases in response to the degradation of the corpus luteum, while its production is stimulated by mifepristone.3,6
Isradipine: Isradipine is a calcium channel agonist that is used to treat preterm labor.7 By blocking voltage-dependent calcium ion channels, isradipine reduces the intracellular concentration of this ion in smooth muscle cells.7 Ex vivo experiments using human uterine tissue found that this drug reduces the frequency and amplitude of spontaneous myometrial contractions.7
Isradipine model
Discover whether your test article affects uterine relaxation via calcium channels, with isradipine as a reference compound.
Isoprenaline: Isoprenaline is a non-selective β-adrenoceptor agonist that is structurally related to adrenaline.8,9 In rats, isoprenaline reduces spontaneous uterine contractility and increases uterine levels of cAMP.10
Isoprenaline model
Discover whether your test article affects uterine relaxation via adrenoceptors, with isoprenaline as a reference compound.
Sodium nitroprusside (SNP): SNP is a nitride oxide (NO) donor that suppresses uterine contractility, however, its mechanism of action is unknown.11 In non-uterine tissues, NO causes smooth muscle relaxation through the accumulation of cGMP via guanylate cyclase, but is more likely to mediate myometrial contraction via changes in calcium ion concentration.11
Sodium nitroprusside (SNP) model
Discover whether your test article affects uterine relaxation via nitric oxide donors, with SNP as a reference compound.
Tocolytics: Tocolytics are commonly used to prevent preterm labor, which is the leading cause of perinatal mortality and morbidity.7,12 You can find out more information about their pharmacology in the video below.
Measuring ex vivo uterine contractility
A key advantage of measuring uterine contractility ex vivo is being able to eliminate species differences. For example, magnesium reduces myometrial contractility in animal and cell models but does not demonstrate the same effects clinically.13 And while relaxin has been shown to inhibit uterine contractility in rats, mice, and pigs, it does not prevent uterine contractility in humans.2
Human tissues can be used ex vivo to more accurately mimic human drug responses in vivo. In these experiments, ethically-donated, living uterine tissue is suspended in an organ bath system. Following functional checks to ensure the tissue is physiologically active, compounds can be added in increasing concentrations while changes in tissue tone are measured - creating a cumulative concentration-response curve (CCRC, figure 1).
If you are interested in learning more about ex vivo uterine contractility models, read our case study describing how experiments in human uterine tissue helped the International Partnership for Microbicides (IPM) gain regulatory approval for their HIV prevention tool.
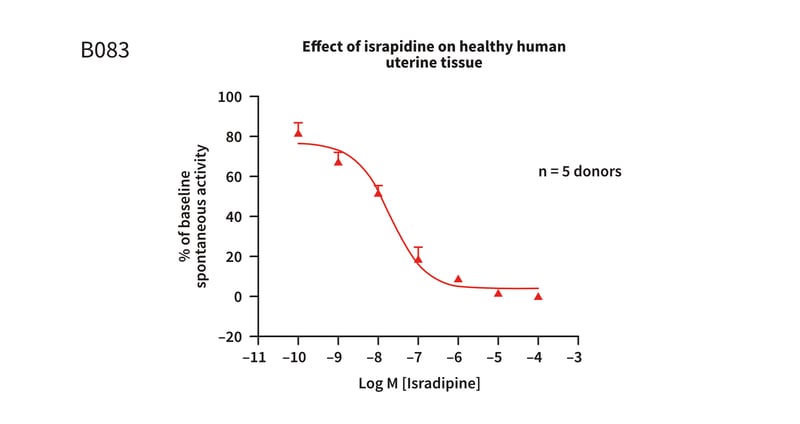 Figure 1: CCRC to isradipine in healthy human uterine tissue, pre-constricted with EC80oxytocin. A concentration-dependent reduction in the spontaneous activity of the tissue is observed.
Figure 1: CCRC to isradipine in healthy human uterine tissue, pre-constricted with EC80oxytocin. A concentration-dependent reduction in the spontaneous activity of the tissue is observed.

References
- Simhan NH et al. Preterm Labor and Birth. Obstetrics: Normal and Problem Pregnancies (2017).
- George AF et al. Female Reproduction. Encyclopedia of Reproduction (2018).
- Ziegler D et al. Pelvic Imaging in Reproductive Endocrinology. Yen & Jaffe's Reproductive Endocrinology (2009).
- Chudnoff S et al. Review of Vasopressin Use in Gynecologic Surgery. Journal of Minimally Invasive Gynecology 19 pp 422-433 (2012).
- Miller WL et al. Disorders in the Initial Steps in Steroidogenesis. Genetic Steroid Disorders (2014).
- Mendiratta V et al. Primary and secondary dysmenorrhea, premenstrual syndrome, and premenstrual dysphoric disorder. Comprehensive Gynecology (2022).
- Kantas E et al. Effect of Magnesium sulfate, isradipine, and ritodrine on contractions of myometrium: pregnant human and rat. Acta Obstetricha et Gynecologica Scandinavia 81 pp825-830 (2002).
- Isoprenaline. Meyler's side effects of drugs (2016).
- Osborne DA et al. Evidence-based evaluation of the management of neonatal shock. Hemodynamics and Cardiology: Neonatal questions and controversies (2008).
- Salveig RM et al. Effects of β-adrenergic agonists on rat uterine motility and cAMP levels in vivo. Acta pharmacologica et toxicologica. 47 pp5-10 (1980).
- Orth TA et al. Additive inhibitory effects of progesterone and sodium nitroprusside on uterine contractility during pregnancy. Reproductive Sciences 18(9) pp868-875 (2011).
- Alexander JM et al. Clinical Management. Chelsey's Hypertensive Disorders in Pregnancy (2015).
- Cuppett CD et al. Uterine Contraction Agents and Tocolytics. Clinical Pharmacology During Pregnancy (2013).

About the author
Zara Puckrin BSc, digital marketing manager, REPROCELL Europe
Zara is a GCU graduate who loves minimalism, marketing, and molecular biology. You can contact her on LinkedIn.
Subjects we write about
- 3D Cell Culture
- Cell Culture
- Central Lab Services
- Clinical Capabilities
- Disease Modeling
- Drug Discovery
- Gene Editing
- Genomic Services
- GMP
- Human Tissue Samples
- Human Tissue Testing
- IBD
- Life Sciences
- Master Cell Banks
- Neurons
- Oligonucleotide Synthesis
- Pharmacology-AI
- Precision Medicine
- Product Catalog
- Regenerative Medicine
- Respiratory Disease
- Safety Pharmacology
- Skin Disease
- Stem Cells
.jpg?width=400&height=225&name=New%20Approach%20Methodologies%20(NAMs).jpg)


.jpg?width=400&height=225&name=Untitled%20design%20(10).jpg)

